- Features
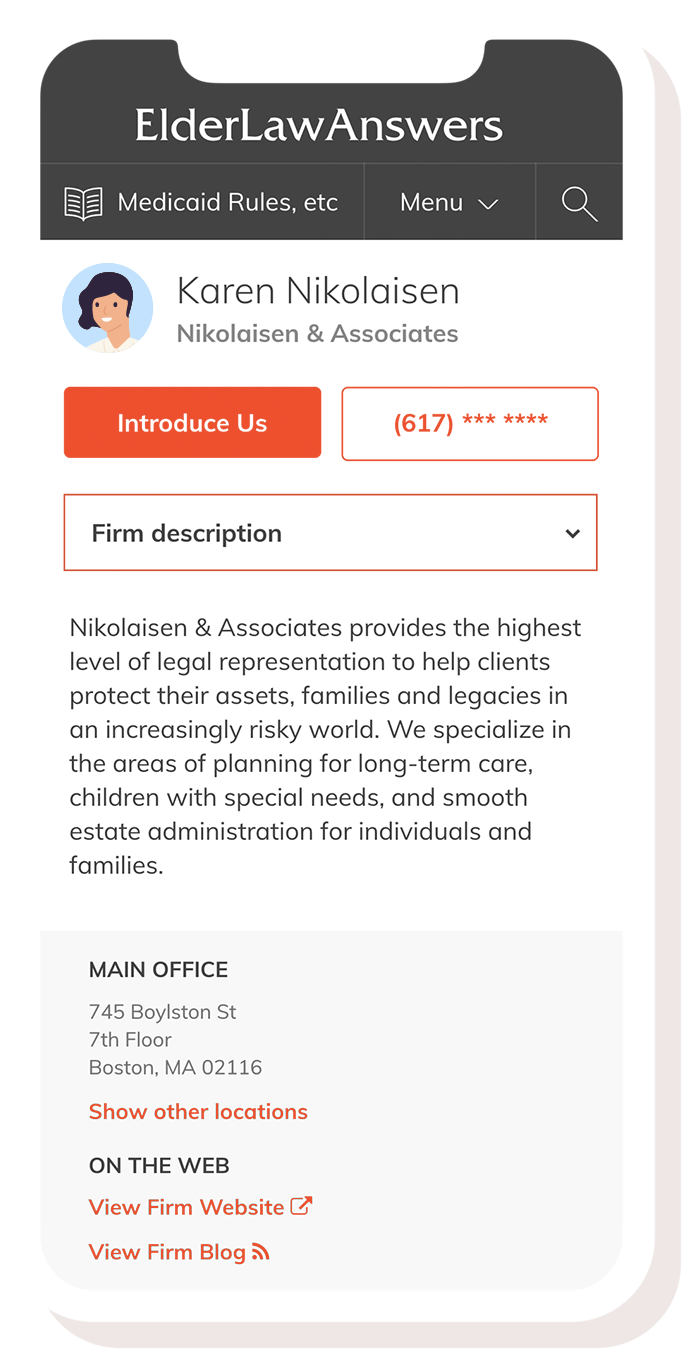
List Your Firm
Get listed in our Online Directory
Send E-Newsletters
Connect. Stay in touch. Promote.
Estate Planning E-Letter
Grow your estate planning practice
Content Marketing
Consumer-oriented elder law content
- Pricing
- Knowledge Bank
Knowledge Bank Search
Search our list of consumer articles
Elder Law Update
Get the latest tips in your inbox
Webinar Registration
See our upcoming elder law webinar
- For Families
- Sign in